There is a difference between the Regulations and mandated Guidelines Vs a manual for inspectors on how to conduct audits and rate Providers
The first carries legal weight, and is the basis of prosecutions, fines, or removal of the licence to trade, whereas the guides are designed to ensure inspectors work in a methodical and consistent manner to form an opinion.
The original “prompts”, the KLOEs, and the Single Assessment Framework fall in the category of internal guidelines for inspectors, however, the conclusions from those can be used to assess whether the Provider was compliant with the regulations.
Quote from the original Essential Standards (2010)
The legal status of our guidance for providers
Although we must take it into account when making decisions about a provider’s compliance with the regulations and in tribunals and courts, the guidance is not enforceable in its own right. In that document, the guides were described as "prompts" to emphasise the fact that these were not part of the regulation.
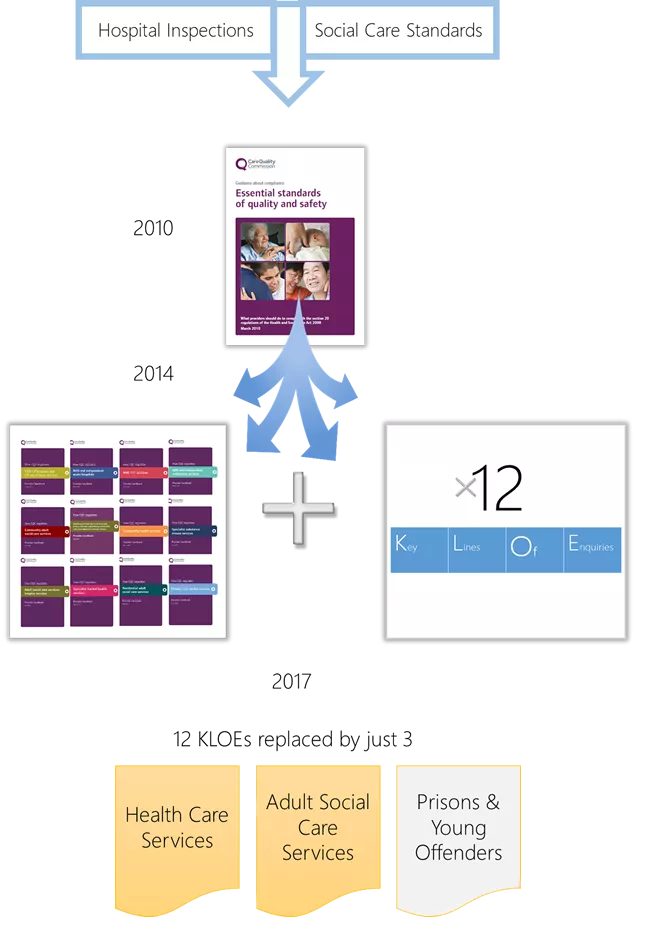
The problem with KLOEs
Health and Social Care Act was not even mentioned in KLOEs
- KLOEs were not regulations
- They had no legal basis
- They were not enforceable
- They were not quoted in inspection reports
If a full inspection was carried out strictly based on all the KLOEs, each inspection would take 10 days or more. Few inspectors, if any, used this as a basis of an inspections.
Single Assessment Framework
Before this Framework, ratings were pure judgement and opinion of the individual inspector.
The main objective of this framework is to standardise and bring some level of consistency to the way inspectors measure and rate each of the Quality Statements.
It is s till an opinion based assessment, but now adds a layer of 6 Evidence Categories, which are given a score and then aggregated.
- The Quality Statement represent what the inspection team will look for
- The related Regulation is identified
- Best Practice is suggested for each
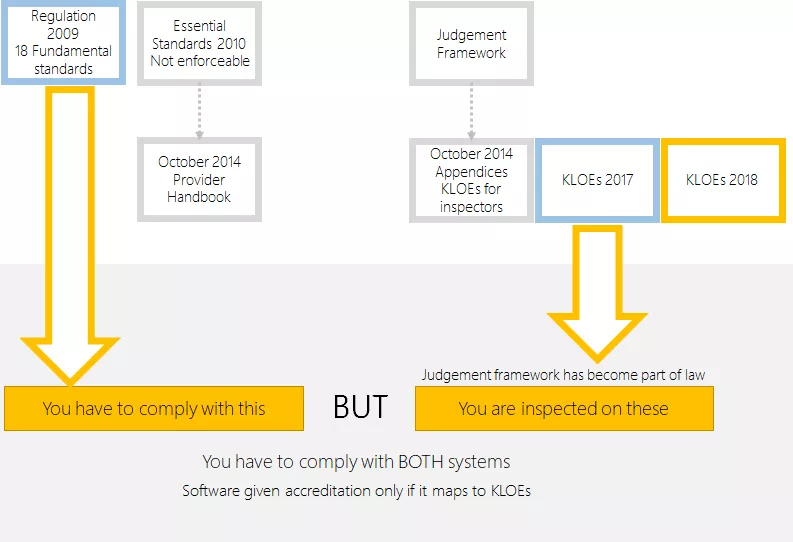
Dilemma for Providers
You have to comply with the HSCA Regulations but you cannot ignore the methodology used by the Regulator to reach their conclusion. In essence, the Provider ends up with having to complying with two sets of rules.
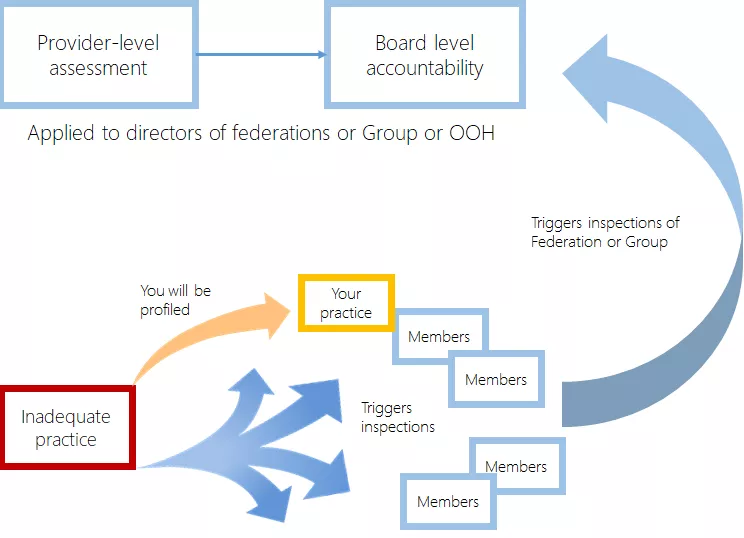
The inspector carries out two separate jobs at an inspection:-
- A subjective rating of your services
- An objective/legal judgement whether you are complying or in breach of the Regulations
Being rated as “inadequate” is not desirable, but only has a direct impact on your registration if you are ALSO found to be in breach of a regulation.