| In a nutshell | |
Expert in a single day:
|
|
| |
|
|
Key takeaways for the Single Assessment Framework |
|
2 to 5 year transition period
|
|
Don’t waste time on learning the scoring system
|
|
There are 15 Frameworks
|
|
One rule for inspectors another for Providers
|
|
Same same but different
|
|
| |
|
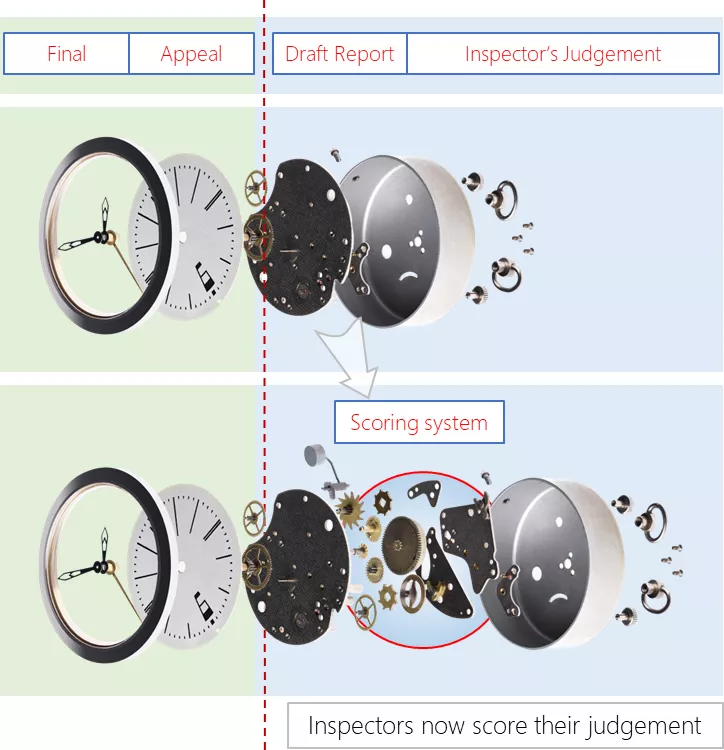
| The scoring system is for Inspectors |
|
 |
|
| The Evidence Scoring System is for Inspectors |
|
In simple terms, instead of looking at evidence and scoring Yes or No for adequacy, an inspector has to look at 6 defined aspects and score them from 1 to 4 to justify their decision. The scoring adds some nuance, but it is still the Inspector's judgement, the same as before. 4 = Evidence shows an exceptional standard |
|
|
Don't waste time trying to understand the scoring system |
Improved scores are only achieved through robust processes and evidence from your governance system and ensuring that this aligns with the Quality Statements. The best time to tackle scores and ratings is at an actual inspection or assessment by engaging with the inspector on how they arrived at the rating. |
What you need to know |
|
What you don’t need to know:- |
|
There are aggregation rules with sub-rules on how everything is added up and weighted. You cannot predict this accurately, and the inspector has leeway to change this depending on their findings and judgement. |
The formulas are not fixed:- |
|
Aggregation: “If we identify concerns during an assessment, we will use our professional judgement to decide whether to depart from applying our ratings principles” Weighting: “We can adjust the following principles for combinations where it is not appropriate to treat ratings equally” |
Old ratings are redundant |
|
The old ratings are not like-for-like, you cannot compare them to new ratings as they are measured completely differently What this means is that a Provider rated as Good might still be Good, but they may well fall short on the new standards, as the focus has changed more towards external feedback from the old site inspections and internal evidence. |
| |
| CQC Scoring and Rating at a glance |
|
In very simple terms, this is all you need to know:-
(By adding up we mean a method of calculating and aggregating is used to arrive at an "average") |
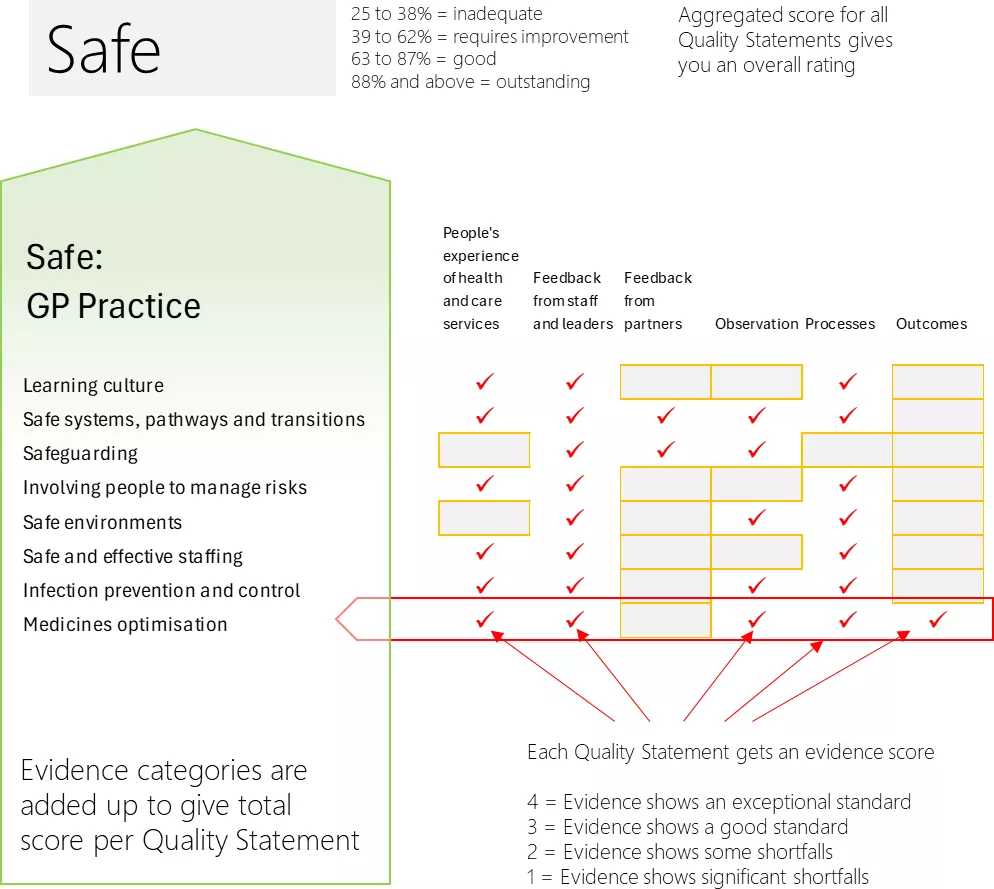 |
| The Evidence Scoring has now been scrapped On 3rd October 2024 the CQC scrapped the "evidence scoring", and will only score the Quality Statements. This does not mean the Evidence Categories are scrapped, merely that the scoring system has been modified. This is not necessarily good news, as the Evidence Categories will still be used but we have lost transparency about how the inspector reached the rating, and we can no longer challenge the weight given to different types of evidence |
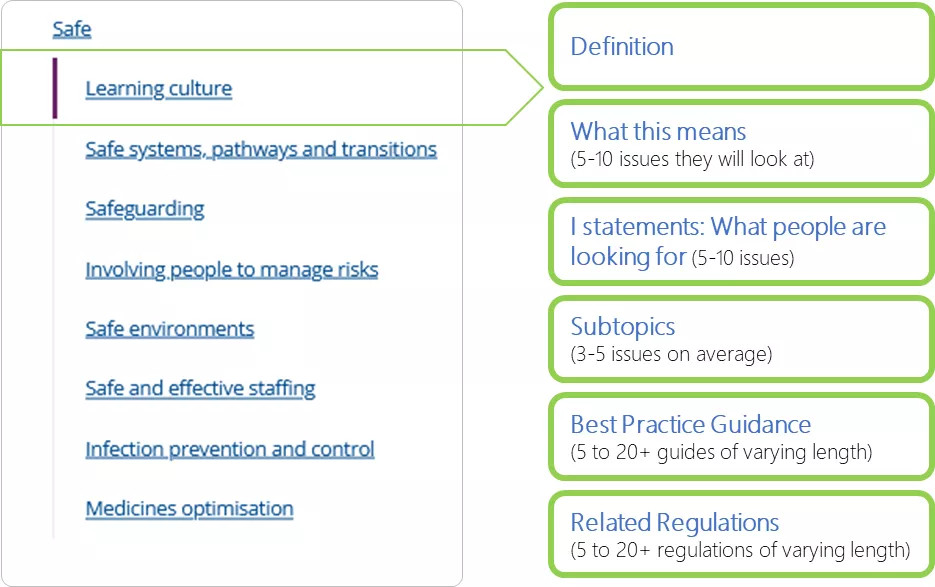
| How Quality Statements are Structured |
| Each Quality Statement has similar components, ranging from a basic definition to the issues the CQC expect to look at together with a link to the Regulations, other legislation and Best Practice Guidance |
 |
| |
Preparation time |
|
If you are not already familiar with the Regulations, the average time you need to reserve to study all the content, including Best Practice and Regulations, can vary between 5 hours for the simpler statements to 15 days for the more complex statements. As an example, Safeguarding lists 16 “Additional legislation” and 27 documents on “Best Practice Guidance”. The CQC states “We expect providers to be aware of and follow the following best practice guidance”, where some documents are more than a hundred pages; making the total reading list in the region of some 3,000 pages on this single Quality Statement. |
The theory: What the CQC expects
|
The challenge: Implementing everythingQuality Statements Policies Processes and Training |
The Practice: What Providers usually doSmaller Providers will generally ignore the official documents altogether and subscribe to a Policies Library service, which gives them access to hundreds of policies containing a standard process. Complex and Enterprise Providers with greater financial resources, have the advantage of being able to engage specialised staff, and devote resources to bespoke documents, processes, and governance systems. |
| Small Medium Enterprises (SMEs) |
|
The Regulatory System does not differentiate between smaller and complex or enterprise Providers. Where an Inspector is familiar with the Provider Type, they will make appropriate adjustments to what can be reasonably expected from an SME. However, it is not uncommon to find an Inspector with a hospital inspection background asking for the same level or Corporate Governance from a sole trader with just 2 members of staff. |
|
The Ratings have not changed, but the way these are determined has changed. Providers will still be rated as Outstanding; Good; Requires Improvement; or Inadequate. However, during the transition period there will be a mix of old and new, until eventually all Providers have been assessed at a Full Inspection under the new rules. |
|
 |
|
| |
|
 |
|
Comparing and Benchmarking |
|
|
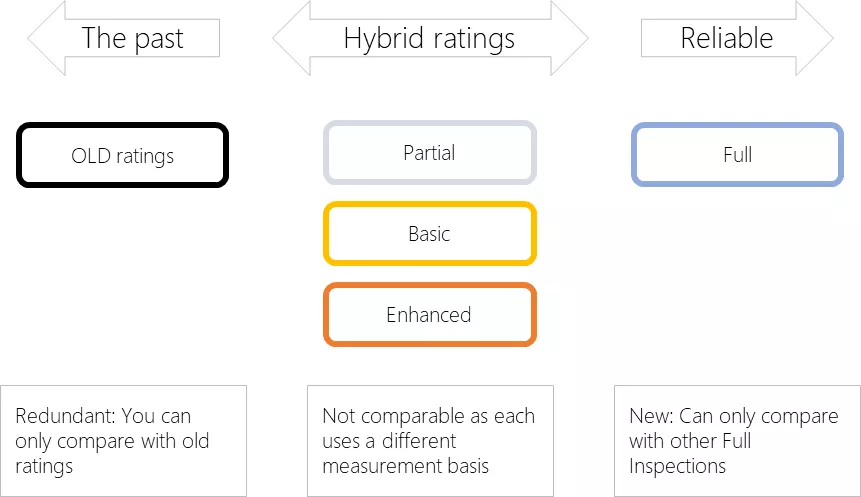
You can only benchmark ratings when they are like-for-like and use the same core measurement criteria. Provider comparison may not be like-for-like. We have identified 5 types of variations that result in hybrid ratings, which will have little statistical or benchmarking value. |
|
| OLD RATINGS |
Old ratings which used KLOEs as the criteria |
| PARTIAL INSPECTION | Inspector reviews one or more targetted Evidence Categories to update an old rating |
| BASIC INSPECTION | Uses Key Evidence Categories from new Assessment Framework (usually around 100 Evidence Category checks) |
| ENHANCED INSPECTION | Uses the Key Evidence Categories as the basis, expanded with additional categories deemed necessary |
| FULL INSPECTION | Comprehensive all 204 Evidence Categories |
|
Reliability of Ratings Benchmarking and comparing Providers is only reliable when each of them have been rated in a full SAF based inspection. Even then, there is likely to a be a level of uncertainty where ratings are based on remote interviews versus an actual site inspection. |
|
Partial Inspection produces a hybrid rating |
|
|
An example of a Partial Inspection is a telephone review of a Provider who was previously rated as Good under the old system. A single or a small number of Evidence Categories such as Equity of Access are reviewed and scored, and all other un-inspected categories are automatically scored as Good on the basis of the previous inspection under the KLOE criteria, which may now be several years out of date. The statistics will incorrectly imply this being a recent Full Inspection. Targetted selection are based on the inspector's judgement. This might be routine or based on new information they have received or where they feel additional reviews are necessary |
|
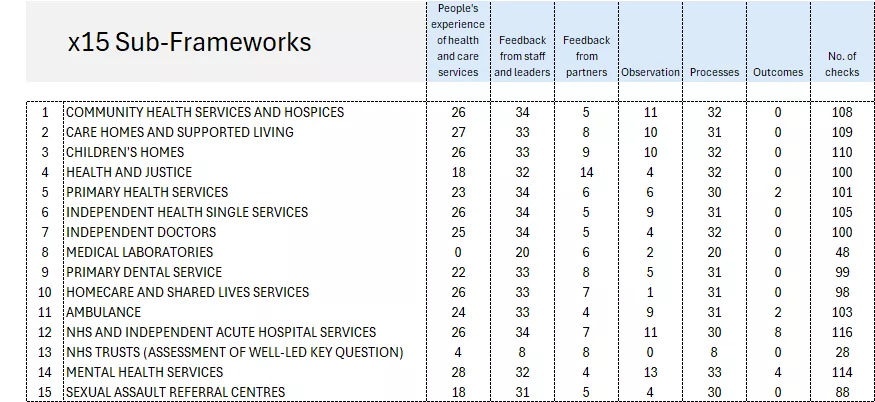
A comprehensive inspection would require 204 checks
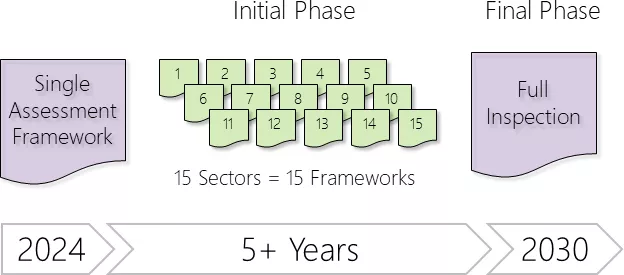
The CQC has adopted a phased approach, with limited checks at the early stages, focused on priority evidence targets. Roughly 100 out of the total 204 evidence categories have been marked as “Key Evidence Categories”. Inspections will focus only on these priority items, but can be expanded during the inspection, if deemed necessary.
Providers were initially broken down into 9 distinct Sectors, now expanded to 15, with variations created for each, resulting in 15 “Single Assessment Sub-Frameworks” until that inspection transitions to a Full Inspection status.
A hybrid system is in place with the following characteristics:-
- 15 frameworks for partial inspections
- Each Sector has different Key Evidence Categories
| Benchmarking |
|
| |
Sub-Frameworks are tailored to each Sector
|
|
|
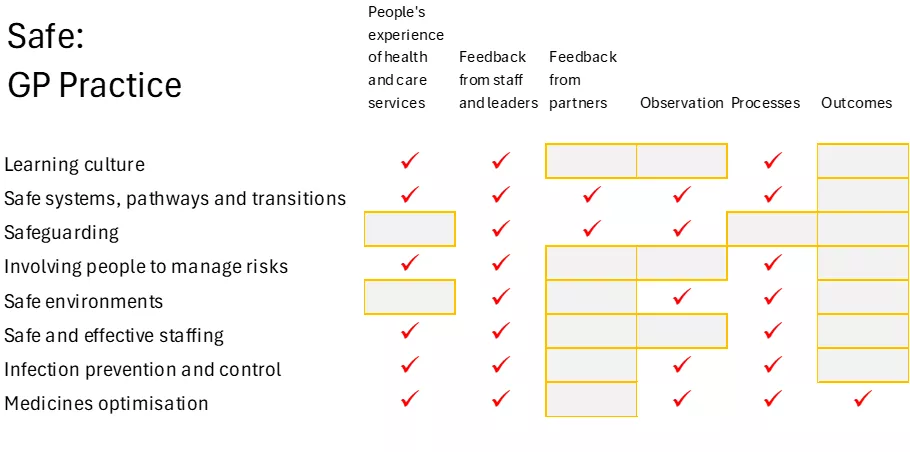
Key Evidence Categories |
|
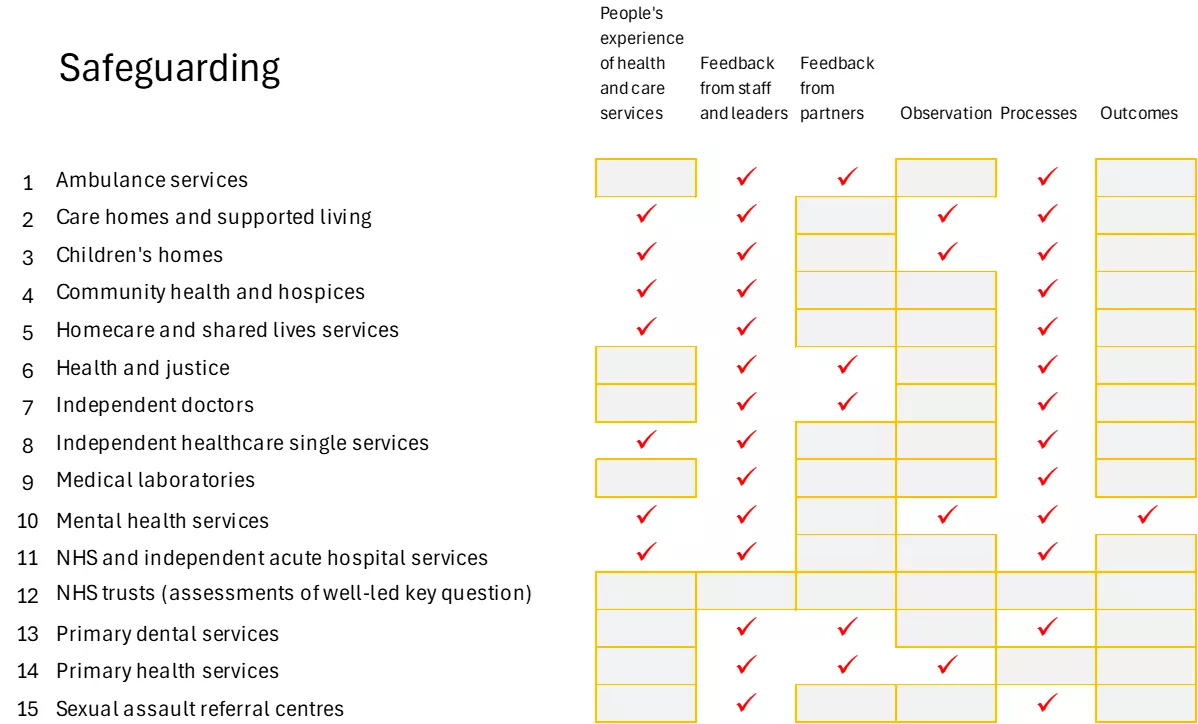
For each sector, a set of Evidence Categories are prioritised as "Key Evidence Categories" which will be checked at the next inspection, the rest are not checked but can be added at the inspector's option. The Key Evidence Categories are different for each Sector |
 |
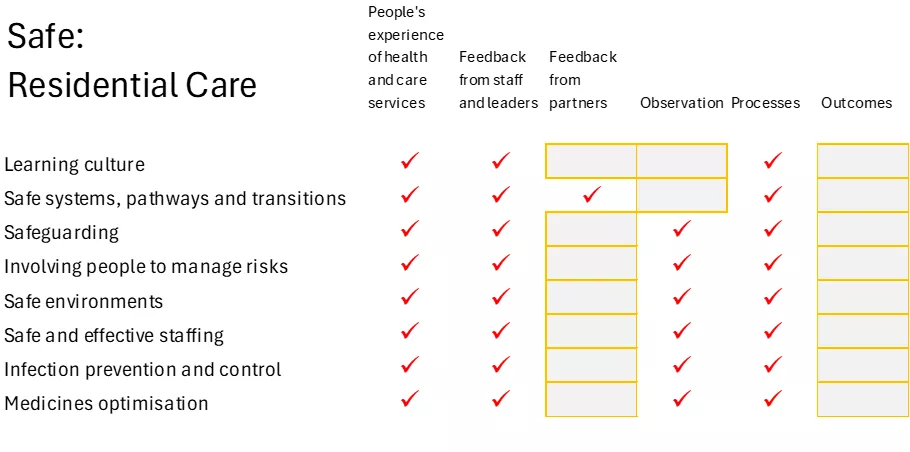
Illustration of variation in Inspection for SAFE
GP Practices Vs Residential Care |
 |
 |
| |
Variation in Inspections for SafeguardingKey Evidence Categories vary for every Sector |
 |
| |
Subcategories
KLOEs blog
Blog appearing under .../Inspections/KLOEs
SOLE TRADERS TO ENTERPRISES
Scalable solutions suitable for Providers of any size and trusted by well known brand names