When it comes to compliance, many practices feel under pressure to keep updating their policy documents year after year. But the reality is very different: regulations hardly change.
The Truth About Policy "Updates"
Most so-called "updates" are minor tweaks—small changes to wording, layout, or grammar. Rarely do they involve substantive legal changes.
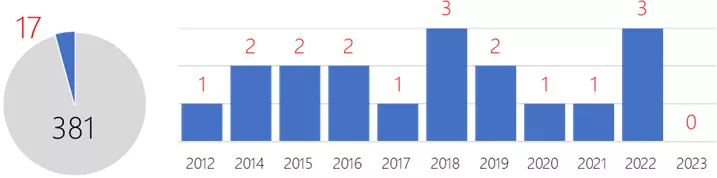
We analysed 10 years of legislation (2012–2023) and found:
- Out of 398 new laws, just 17 affected providers.
- That averages only 1 or 2 meaningful changes per year.
- In 2023, there were no relevant new laws at all.
Key Legislative Changes Since 2012
Here are the substantive changes that actually matter for providers:
| Legislation | Year | Relevance |
|---|---|---|
| Health and Care Act | 2022 | All Providers |
| Approved Premises (Substance Testing) Act | 2022 | Substance Abuse |
| Down Syndrome Act | 2022 | All Providers |
| Botulinum Toxin and Cosmetic Fillers (Children) Act | 2021 | All Providers |
| Coronavirus Act | 2020 | All Providers |
| Mental Capacity (Amendment) Act | 2019 | All Providers |
| Organ Donation (Deemed Consent) Act | 2019 | Hospitals |
| Health & Social Care (National Data Guardian) Act | 2018 | All Providers |
| Mental Health Units (Use of Force) Act | 2018 | Hospitals |
| Assaults on Emergency Workers Act | 2018 | Ambulance |
| Children and Social Work Act | 2017 | Adult Social Care |
| Immigration Act | 2016 | All Providers |
| NHS (Charitable Trusts Etc) Act | 2016 | Hospitals |
| Health Service Commissioner for England (Complaint Handling) Act | 2015 | All Providers |
| Health and Social Care (Safety and Quality) Act | 2015 | All Providers |
| Care Act | 2014 | All Providers |
| Immigration Act | 2014 | All Providers |
| Mental Health (Approval Functions) Act | 2012 | All Providers |
That's it. Fewer than 20 laws in a decade have made a real difference to provider compliance obligations.
What Suppliers Won't Tell You About Costs
The compliance market is big business. Providers are often sold more than they need. Here's what's typically on offer:
What's Available
- Downloadable packages – around £300 or less, promising 500+ policies, procedures, letters, and templates.
- Online systems – £1,000–£2,000 per year, offering over 1,000 pages of guidance, with features like staff activity logs.
The Hidden Costs
- Time to read every policy: Between one and three months of solid work (most never attempt it).
- Staff training/testing via online systems: Adds administrative load and ongoing management time.
- Briefing and testing staff knowledge: For a small organisation, this can equate to £15,000 in annual costs.
Saving Time and Money
Here's the bottom line:
- Suppliers have little incentive to tell you the truth. If they admitted you only need 50 core policies, and that legislation changes maybe once a year, their model collapses.
- You do not need a policy for every occasion. A well-written standard policy, applied with common sense, usually covers most scenarios.
- Use policy packages selectively. If you're buying a large library, treat it as a reference resource—not a manual that must all be implemented.
Key Takeaway
Regulations are relatively stable, and the real compliance burden is often overstated. Instead of drowning in hundreds of documents, invest in a concise set of core policies, keep an eye on genuine legal changes, and focus on training staff to apply good judgement.
In other words: compliance is about people, not paperwork.
Would you like me to combine this with the previous blog (on number of policies) into a longer guide-style article, or keep them as two separate, more focused posts?
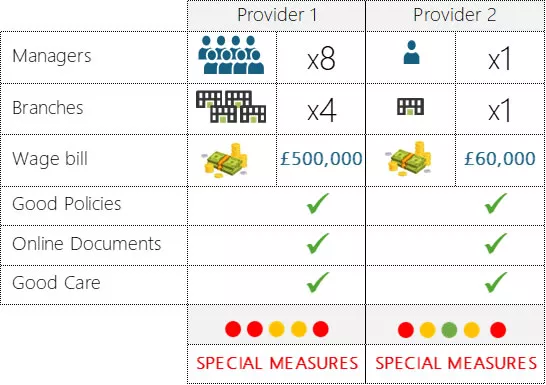
How these providers failed at everything all at once
We looked at two particular inspection failures, one had as many resources as you could wish for and another being your usual smaller provider with one Manager.
Both had comprehensive policies; an online document management system; and generally provided good care.
Things ran smoothly. Everything looked fine.
At The inspection
It all looked good on paper, so the CQC Rating came as a shocker.
Senior Management is shocked!
Information isn’t to hand, processes are not always followed, there are gaps in the system, things are not done properly.
2024 Inspections will be even more challenging as the focus shifts to “Feedback” which most systems are not designed for
This rating will stay on their web site until the next inspection. That could be the next 5 Years, unless you ask for a reinspection.
Lessons learnt
- It is not just about having the best policies or more human resources
- 99% of the inspection is about continuous compliance
- Don’t let the inspector be the first to find your weaknesses
The solution
CQC inspections are based on your performance over the last 12-24 months. By the time an inspection is announced, it is already too late to prepare.
The registered Manager is central to an inspection. The uncomfortable truth is that the Registered Manager delegated everything, did not monitor, and took their eye off the ball.